
In 2013, 246 Canadians died waiting for organ transplants.

They needn’t have. There’s no shortage of organs that could be used to save those individuals, if only their owners would volunteer their transplantation while still alive.
Instead, when the vast majority of Canadians die, the body parts on which they relied while alive, which could go on to save or drastically ameliorate the lives of desperate strangers, get buried or cremated with them.
It’s not because of a disproportionate opposition among Canadians to donating body parts. It’s because, many times, individuals die in hospital and no one follows up to recover vital organs and tissue.
Canadian transplant methods are reaching a level of space-age sophistication, employing world-class innovative tools to make the most of the body parts at their disposal.
But, the waiting list for viable kidneys, lungs, livers, hearts remains stubbornly long. There still aren’t enough donated body parts to go around.
About one per cent of Canadians who die in hospital donate an organ. It works out to about 15 per million – about half the rate of countries such as Spain (34 per million) and the United States, at 26.
So what gives?
Organized donations
The secret to getting more organs donated may not lie in convincing more people to register as donors, said Steven Paraskevas, Director of McGill University’s Pancreas and Islet Transplant Program and president of the Canadian Society of Transplantation.
Rather, the key change comes postmortem.
You need trained personnel assigned to hospitals’ Intensive Care Units whose job it is to identify deceased people who could donate organs and approach grieving relatives to obtain their consent.
The concept – taking advantage of every potential donor – is simple. But its execution is not: It requires changing the way hospitals operate, Paraskevas said.
“It really depends on the system, and who is doing the asking, and how its being done, and whether they find cases where organ donation potentially exists.”
And while the creation of these dedicated teams costs money, he’s convinced you’d soon make the money back in kidneys alone.
“Canadian public opinion is overwhelmingly in favour of organ donation. … I think the system has been underfunded to take full benefit of that great goodwill.”
It’s also easier said than done to roll out this setup across 10 provinces, he noted.
Ontario, for its part, began mandatory reporting of people deceased or about to die at participating hospitals to the Trillium Gift of Life Network in 2006, the transplant organization says. It now has 62 reporting hospital corporations, with reporting rates ranging from 68 per cent at the Hôpital Montfort and 100 per cent at the Ottawa Heart Institute and the Children’s Hospital of Eastern Ontario.

Get weekly health news
Transplant nation: By the numbers
In the meantime, thousands wait for vital body parts. As of April 23, there were almost 1,600 people in Ontario on organ waitlists.
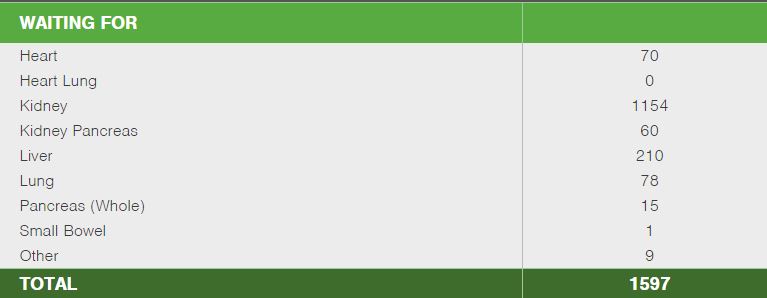
Source: Trillium Gift of Life Network
In 2013, surgeons across the country performed 2,367 organ transplants, according to the Canadian Organ Replacement Register:
- 1,419 kidneys
- 509 livers
- 247 lungs
- 192 hearts
- 65 pancreases
Just under half of that year’s donors were deceased. But a dead person can give far more organs than a living donor, who still needs them.
The rate of donors varies significantly by region: Quebec had the most deceased donors in 2013, with 20.2 per million population (Manitoba and Saskatchewan, on the other hand, had only 7.2). British Columbia is Canada’s living donor capital, with 28 living donors per million people.
In theory, the more you can take advantage of organs from deceased donors, the less you need to rely on living ones.
In the meantime, the international transplant community has been roiled by questions of whether there’s an ethical way of providing incentives for people to donate.
Last June, a coterie of medical professionals from the U.S. transplant community met to discuss just that. There’s no shortage of grey areas: Ensuring all living donors are compensated not only for direct costs (such as travel) but also any wages lost as a result of the surgery seems like a no-brainer but can be tough to calculate. Immediate post-surgery health care is one thing, but should a living donor get lifetime health insurance, or is that an unethical incentive?
Organ donation: Everything you wanted to know (but were afraid to ask)





Graphic by Leo Kavanagh, Global News
When a person dies in hospital, the individual is kept on a ventilation unit that keeps blood flowing through organs even after the brain’s deceased.
It’s ultimately up to the person’s next of kin to decide whether his or her organs can be transplanted, although staff at Ontario’s Trillium Gift of Life Network said they usually comply with a designated organ-donor’s wishes.
Once health care practitioners get the okay, they set to work assessing whether the donor’s organs and tissue can be transplanted. They’ll check a person’s medical history and order ultrasounds and bloodwork on each organ. This can be more complex than you’d think: If a donor’s in Thunder Bay and you want to run a bloodwork check on transplantable organs, those blood samples may have to hop a ride on a commercial airline (or hitch a ride on the road with Ontario Provincial Police) to Toronto to be processed.
Health Canada sets the rules regarding what’s transplantable and what isn’t. Very few medical conditions completely rule out organs as potential transplants: It all depends on the organ and on the person who needs it. Rabies is exception: Individuals with rabies can’t donate. A history of cancer may or may not rule out transplant options, depending whether the cancer metastasized, whether it’s been in remission and for how long, what body part or parts were affected. Blood-borne diseases such as HIV or hepatitis nix tissue, but not organ transplants.
And even if it looks at first blush like an organ isn’t doing too well, health care teams will go back periodically to check and see whether there’s been an improvement. (Crazy as it sounds, your body parts – if hooked up to an IV and properly cared for – could actually start functioning better hours after you die.)
It’s ultimately up to transplant teams whether or not an organ can be used.
There’s a specialized team for each transplantable organ – heart, lungs, liver, kidneys, pancreas, small bowel. They will travel to the donor and take turns recovering their respective organs, then take the organs back to the transplant team’s institution to conduct surgery on the recipient.
Even then, there can be complications. But the medical profession is getting better at finding matches and ensuring a recipient’s body will accept and work with the new body part.

Graphic by Chris Jeri, Global News
Comments
Want to discuss? Please read our Commenting Policy first.