Watch above: Dr. Ali Zenter explains how the common practice of taking an aspirin every day to prevent heart attacks has been called into question.

It’s been almost 20 years since I started medical school. I remember my first class on heart disease.
It was taught in a tutorial, small group setting with the principles of problem based learning.
We discussed a case based on a 67-year-old man who had high blood pressure and took Aspirin to prevent a heart attack.
I remember that case as if it were yesterday.
The class is long gone and the patients are now very real, but the principle of prevention remains.
Prevention comes in many forms. In medicine we tend to break prevention down into primary prevention, meaning preventing your first event, and secondary prevention, preventing your second event.
Whether it is primary or secondary prevention, it’s always important to weigh the risk of prevention against the benefit.
READ MORE: Do you have atrial fibrillation? What you should know about treatment
Sometime we use behaviours to intervene — as with diet, exercise and smoking cessation — and sometimes we use drugs.
As far as drugs go, Aspirin is an icon: It’s been around forever and it is universal.
You can walk into any pharamacy in the world, ask for Aspirin and, I would argue, you’ll likely find it.
It is a staple in most medicine cabinets and first aid kits. I’ve even seen it served standard in hotel mini-bars next to the $8 peanuts.
Aspirin has a long history in the world of cardiovascular disease prevention.
Since the late 1970s, there have been over a dozen secondary prevention trials showing the benefits of Aspirin use in the treatment of heart attack and strokes, and in the treatment of people with a history of heart attacks and strokes.
There is no debate that if you are having a heart attack or a stroke an Aspirin may save your life.
Similarly, there is no debate that if you’ve had heart disease — a heart attack, angina, angioplasty or bypass surgery — or if you’ve had a stroke or a warning stroke (TIA), an Aspirin may save your life.
But what about if you’ve never had a heart attack or a stroke?
What if you are, let’s say, a 60-year-old healthy man or woman? Do you take an Aspirin a day to prevent your first heart attack or stroke?
Twenty years ago, as your doctor, I might have told you “yes.” Today, my answer would be much different.
READ MORE: Dr. Ali Zentner on homeopathy: ‘I only speak the truth’
The first prevention trials on Aspirin came to light in the late 1980’s.
Some of the studies were not placebo-controlled, and the patient population was variable from low to moderate risk.
The dose of Aspirin also varied among the trials.
In total there are nine large primary prevention trials looking at Aspirin’s role in prevention of cardiovascular disease.
The issue with the trials is that there is indeed such a diversity among them; the populations are different, the doses of Aspirin used are variable and women are very poorly represented.
The data shows that if you treated 1000 patients per year with Aspirin, you avoid about twi vascular events (heart attacks or strokes).
The secondary prevention data is different.
Low-dose Aspirin has been shown to be effective in preventing about 50 per 1000 patients per year of cardiovascular events (non-fatal myocardial infarction, non-fatal stroke, or vascular death) in a meta-analysis of 16 secondary prevention trials in patients with previous cardiovascular disease.
Three large meta-analysis of the primary prevention data further show a rather weak argument for Aspirin use in primary prevention patients.
The data from one such meta-analysis, called the Antithrombotic Trialists looked at six randomized primary prevention trials. It concluded that you need to treat about 2000 low-risk people with Aspirin for at least three years to prevent one non-fatal heart attack.
Further meta-analyses confirm this weak picture for Aspirin in primary prevention in patients with diabetes who have never had a heart attack.
The real issue is that Aspirin itself is not without risk. The same prevention data shows that for every 1000 people taking Aspirin, one will have a gastrointestinal bleed.
As a doctor, I weigh risk and benefit every day.
When it comes to Aspirin use, the table below speaks volumes on summarizing the risks and benefits according to the evidence.


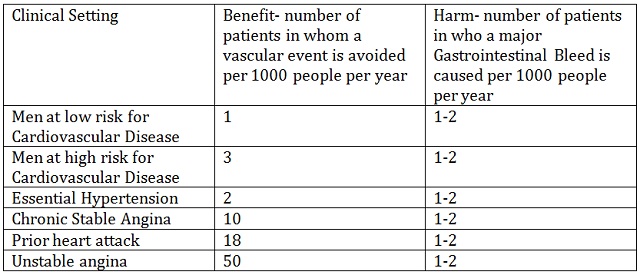
If you are a low-risk man, the benefit of taking an Aspirin a day to prevent a heart attack is lower than the risk of a GI bleed.
For a high-risk man, the risk is about the same.
For women, the data shows that the risk of GI bleed is higher than the benefit.
I think future studies will continue to support this as we continue to improve upon the treatment of risk factors for cardiovascular disease.
The landscape of prevention continues to change.
We are indeed better at controlling risk factors for heart disease and stroke. As we continue to improve, I suspect Aspirin will play less of a role in the primary prevention picture.
I can’t stress enough that this is in the primary prevention population.
If you’ve had a heart attack, a stroke, angioplasty, or have known cardiovascular disease please don’t stop your Aspirin. In fact, don’t do anything without talking to your doctor.
In medicine as in life, things work best when we adapt to change.
Think about it for a moment- the human race has gotten to where it is based on this principle. Evolution itself really is adaptation on a grand scale.
I realize I may be off on a philosophical tangent, but it’s Monday and I am amazed at how my profession continues to evolve in the 20 years since I walked into my first medical classroom.
No doubt the debate will continue as more studies come to light.
For now, I agree with the FDA and their refusal to approve Aspirin for use in primary prevention of cardiovascular events. The science as it stands now supports this recommendation.
Dr. Ali Zentner is the medical consultant for Global National’s “Health Matters” segment.
Referrences:
- Baigent C, Blackwell L, Collins R, Emberson J, Godwin J, Peto R, Buring J, Hennekens C, Kearney P, Meade T, Patrono C, Roncaglioni MC, Zanchetti A. Antithrombotic Trialists’ (ATT) Collaboration. Aspirin in the primary and secondary prevention of vascular disease: collaborative meta-analysis of individual participant data from randomised trials. Lancet 2009;373:1849–1860.
- Patrono C, García Rodríguez LA, Landolfi R, Baigent C. Low-dose Aspirin for the prevention of atherothrombosis. N Engl J Med 2005;353:2373–2383.
- The Medical Research Council’s General Practice Research Framework. Thrombosis prevention trial: randomised trial of low-intensity oral anticoagulation with warfarin and low-dose aspirin in the primary prevention of ischaemic heart disease in men at increased risk. Lancet 1998;351:233–241.
- Carlo Patrono, Eur Heart J. 2013;34(44):3403-3411.Low-dose Aspirin in Primary Prevention Cardioprotection, Chemoprevention, Both, or Neither?
Comments